
Frequently Asked Questions
- What could be wrong?
- What happens in an ART (Assisted Reproductive Technology) cycle?
- Is there a psychological impact of IVF?
- What is ICSI?
- What is Assisted Hatching?
- What is Endometriosis?
- Is there a higher rate of multiple births while undergoing IVF?
- Are the chances of the child having birth defects increased?
- Are there any restrictions on physical or personal activities during an ART cycle?
- What happens if I become pregnant?
- If I am not pregnant, when can we try again?
- How do we decide how many embryos to transfer?
- Am I depleting my store of eggs by doing an ART cycle?
- What would you say is the number one most important thing a couple should do first in seeking out treatment??
- The second most important thing?
- What has the highest success rate for couples just starting out?
- How long should a couple stay on a regimen before it’s effectiveness rules it out? For example: Some doctors advise that if you haven’t gotten pregnant after 3 rounds of Clomid, you should move on. Is this timeframe the same for most of the procedures?
- Money and stress are important factors. Any tips on how to keep the stress level from getting so high, it adversely effects a couple’s health, and thus the ability to get pregnant?
- Is there ever a point where you would advise a couple to stop pursuing therapies?
What could be wrong?
 Male and female factors can equally be the cause of infertility. Approximately 40% of the time the infertility is the result of a male factor and 40% of the time it is the result of a female factor. In 20% of cases, both male and female factors are involved.
Male and female factors can equally be the cause of infertility. Approximately 40% of the time the infertility is the result of a male factor and 40% of the time it is the result of a female factor. In 20% of cases, both male and female factors are involved.
It is imperative that you undergo a complete infertility evaluation before speculating on the causes and treatments. This information is not a substitute for a physician consultation or infertility evaluation. It just provides some insight into the common diagnoses.
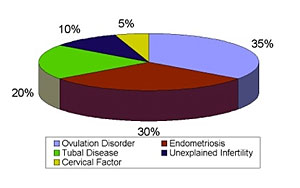
The typical causes for female infertility and the rough percentages that they occur are graphed below. Please contact LifeStart Fertility Center for more information and to set up an appointment with Dr. Singh for an infertility evaluation.
What happens in an ART (Assisted Reproductive Technology) cycle?
A cycle begins with the administration of fertility drugs. This is called controlled ovarian hyperstimulation. The goal is to produce multiple follicles on the ovaries from which eggs are retrieved. The specific fertility drug protocol utilized varies and is individualized for each patient. Most of the medications used are for the female; however, the male is asked to comply with a regimen of antibiotic therapy to prevent and treat certain organisms in the semen that can lower fertility success rates.
Transvaginal ultrasound examinations and blood estradiol levels are used to monitor follicle growth and egg development. As the follicles in the ovaries grow, they produce increasing amounts of estradiol. The physician compares the estradiol level with the ultrasound results to determine if any medication adjustments are necessary. The physician also uses this information to determine the most optimal time to proceed with egg retrieval.
A baseline ultrasound and estradiol level is obtained prior to beginning any stimulation medications. A repeat ultrasound and estradiol level is usually obtained on stimulation day six. Eventually, ultrasound examinations and blood tests may be necessary on a daily basis. The ovarian stimulation is usually about 9 to 12 days.
Controlled ovarian hyperstimulation ends when the physician determines an appropriate number of eggs are likely to be mature (based on ultrasound and blood test results). All fertility-stimulating drugs are discontinued at this time. The patient administers an hCG (PregnylTM or ProfasiTM) injection at a specific time as instructed by the physician. Oocyte (egg) aspiration is scheduled 36 hours following the hCG injection.
A small percentage of patients who begin taking fertility stimulation medications have their cycle cancelled before any procedure is done. The reasons for cycle cancellation can include an insufficient number of mature follicles, an inadequate blood level of estradiol, or an exaggerated response leading to a risk for hyperstimulation syndrome. If an ART cycle is cancelled, medications may be modified in subsequent attempts in order to try to improve the response.
Is there a psychological impact of IVF?
Those couples that do not conceive with basic fertility treatment modalities find themselves confronted with decisions concerning In Vitro Fertilization (IVF). Assisted Reproductive Technology may cause additional stress for couples that have already endured multiple disappointments. IVF can be difficult, both physically and emotionally. Studies have shown that couples that know what to expect are better able to endure these processes and use their own natural coping skills to their best advantage.
- For many couples this is the last step toward achieving a biological child.
- It is difficult to realistically confront the odds while remaining optimistic enough to endure a regimented treatment program.
- An IVF treatment cycle disrupts work, school and daily schedules.
- Physical distance from an IVF program may cause daily commuting, separation from the spouse if commuting is unrealistic, or additional expense and unfamiliar accommodations during treatment.
- A normal grief reaction is inevitable if pregnancy does not occur.
- Joy verses fear can occur when pregnancy occurs and the possibilities of miscarriage or tubal pregnancy remain a threat.
There are several strategies that can assist couples during this time:
- Become informed about IVF.
- Understanding the process of IVF and knowing what to expect will lessen your anxiety about the procedure.
- Be realistic about your expectations. The chance of establishing a pregnancy is 20% to 60% each treatment cycle. Also, each cycle contributes valuable information that can be of assistance in subsequent cycles.
- Set limitations.
- Make decisions ahead of time. Discuss with your spouse your feelings about cryopreservation, donor semen, the number of cycles you will attempt, and who will be included in your confidence.
- Provide for emotional support. Talk about your feelings.
- Keep life simple. Plan activities that are relaxing and entertaining. If you are staying in a hotel, bring familiar items from home.
- Counseling may be of assistance to some couples to help them cope with difficult emotions and stress.
What is ICSI?
ICSI or Intracytoplasmic Sperm Injection is an additional component of an IVF cycle usually used with male factor issues or when fertilization does not normally occur. The procedure, done in the IVF laboratory, takes one sperm and injects it into one egg. This is done with sophisticated magnification and handling equipment. This procedure obviously enhances fertilization rates. For more information about the ICSI procedure, please click here.
What is Assisted Hatching?
Assisted Hatching is a form of embryo micromanipulation that involves the creation of an opening in the outer covering, or zona pellucida, of the embryo. The procedure helps a normal, growing embryo hatch from the covering and implant in the uterus. This procedure may increase the implantation rate, especially in older women. For more information, please visit our Assisted Hatching section.
What is Endometriosis?
The formal definition of endometriosis is endometrium in an ectopic location that contains endometrial glands and stroma. In other words, it is uterine-like tissue that is growing outside the uterus causing pain and/or infertility. Its cause is unknown. There are many theories, but every answer has contradictions. It could be genetics. It could be retrograde menses, menstruation that goes backwards through the tubes into the abdomen. It could be congenital. It could be immunological. It could be all of the above or none of the above. We simply don't know.
Endometriosis is common. The generally accepted percentage of women with Endometriosis is 5% to 15%. However, the true incidence is probably even higher. Many women have Endometriosis and don't have the symptoms (usually pain) or the pressing need to be diagnosed (usually infertility). Endometriosis can be classified as very mild to severe. There are likely many more women with very mild Endometriosis, which does not cause any symptoms.
The only way to diagnose Endometriosis with complete accuracy is to see it. The only way to see it is through surgery (laparoscopy). There are symptoms and tests that can give a physician clues, but Endometriosis is a very elusive disease. The adage "seeing is believing" is the safest and most effective route to pursue diagnosis and ultimately treatment. For more information on endometriosis, please click here.
Is There a Higher Rate of Multiple Births While Undergoing IVF?
There is a higher rate of multiple births for women treated with fertility drugs than in the general population. The actual rate depends on the type of drugs used and the chosen procedure. There are many strategies to minimize the risk of multiple births, but it is always a risk to some degree.
There are three basic types of therapy that increase the risk of multiple births. They are:
- Ovulation induction with Clomiphene
- Ovulation induction with gonadotropins
- IVF procedures with fertility drugs
For more information on which procedure would best fit you, please contact us for a consultation.
Are the chances of the child having birth defects increased?
There is no reported correlation between babies conceived with medical intervention and birth defects. The risk is no greater than in the normal population. These are real and natural babies conceived with a little assistance.
Are there any restrictions on physical or personal activities during an ART cycle?
Yes, there are a number of them.
- Smoking: Stop smoking before treatment begins. If you cannot stop "cold turkey," make an effort to stop at least two weeks before the egg aspiration. Smoking can affect ovarian stimulations, egg and embryo quality, and the likelihood of conceiving.
Numerous studies have demonstrated that smoking during pregnancy can lead to reduced birth weight and fetal compromise. There is some data to suggest smoking can also lower pregnancy rates. New medications are available that can help many people overcome the smoking habit. We strongly recommend that all women, especially those undergoing fertility therapy, cease smoking.
- Drinking: Alcohol is a drug and, in general, should be avoided during infertility treatment and pregnancy. There is no reason to consume alcohol and it can introduce another "unknown" factor into treatment. If you drink socially, you may continue to do so during the controlled ovarian stimulation phase. Two to three alcoholic beverages per week is acceptable. Please do not drink alcoholic beverages from approximately 4 days before egg aspiration until the pregnancy test.
- Medications: If you are taking any medication, prescribed or over the counter, please inform your physician. Some medication should not be taken before an operation, some may interfere with those prescribed during your cycle, and others may interfere with ovulation or pregnancy implantation.
- Your physician will prescribe a multivitamin.
- Inform your physician of any changes in your health even minor colds or infections.
- An ART cycle can be stressful physically and emotionally. Avoid becoming tired in the days before and after a procedure. Eating correctly, and getting proper rest are important.
- An ART cycle can be an emotionally stressful time for you and your partner. You need to consider supportive relationships, for example; friends, clergy, family members, and psychologists.
- Heavy exercise such as aerobics, jogging, weight lifting, roller blading, etc. will be prohibited during ovarian stimulation and until the pregnancy test.
What happens if I become pregnant?
If pregnant, you are asked to return to the office for repeat blood tests and ultrasounds to insure an ongoing successful pregnancy. After approximately 8 weeks, you are referred to an obstetrician for the remainder of the pregnancy.
If I am not pregnant, when can we try again?
Cycles can be done back to back but usually we ask the patient to wait one complete menstrual cycle before beginning another ART cycle. This gives us time to "regroup", evaluate what was learned from the prior cycle and determine the next steps. Sometimes tests are required that can delay subsequent cycles
How do we decide how many embryos to transfer?
Dr. Singh will discuss this with you, but we usually follow the American Society for Reproductive Medicine Guidelines: under 35 years old - 2 embryos; 35-37 years old - 2 or 3 embryos; 38-40 years old - 3 or 4 embryos. The number may also vary depending on each individual clinical circumstance.
Am I depleting my store of eggs by doing an ART cycle?
A woman is born with a full complement of eggs. There are far more eggs than will ever be used during a normal lifetime and ART have no measurable "lowering" effect.
What would you say is the number one most important thing a couple should do first in seeking out treatment?
It is important for them not to wait for help longer than they need to. Women younger than 35 years of age should seek advice after one year of unprotected intercourse while women over age 35 should consult a doctor after 6 months of trying.
What is the second most important thing a couple should do?
They should consult a qualified physician as early as possible and consider seeing a Reproductive Endocrinologist.
What has the highest success rate for couples just starting out?
Success rates are variable depending upon multiple factors including female age and the cause of infertility. Overall, In-Vitro Fertilization (IVF) has the highest success rate amongst current available reproductive technologies.
How long should a couple stay on a regimen before it’s effectiveness rules it out? For example: Some doctors advise that if you haven’t gotten pregnant after 3 rounds of Clomid, you should move on. Is this timeframe the same for most of the procedures?
Once again, each patients case is unique and the # of “rounds” recommended depends on multiple factors including age and cause of infertility. In general, three to four cycles of any ovulation induction regimen done under proper monitoring are reported to have maximum effectiveness.
Money and stress are important factors. Any tips on how to keep the stress level from getting so high, it adversely effects a couple’s health, and thus the ability to get pregnant?
First, thoroughly understand your particular case and cause of infertility. Explore the possible treatment options and select the treatment plan only after a thorough review with a specialist. Make yourself aware that infertility treatments often tend to run a long course. Take advantage of infertility support groups and counselors/psychologists specializing in the area of infertility.
Is there ever a point where you would advise a couple to stop pursuing therapies?
This is a difficult question to answer, as each patient’s situation is unique. If the couple has gone through multiple failed ART (Assisted Reproductive Technology) cycles and if they are not open to egg, sperm or embryo donation as indicated, then adoption should be considered.
